Cite
Mao, Alice R., Matthew Brams, Thomas Babcock, and Manisha Madhoo. “A Physician’s Guide to Helping Patients with ADHD Find Success in the Workplace.” Postgraduate Medicine 123, no. 5 (September 2011): 60–70. https://doi.org/10.3810/pgm.2011.09.2460.
Jeremy
Synth
Contribution::
Related::
Md
FirstAuthor:: Mao, Alice R.
Author:: Brams, Matthew
Author:: Babcock, Thomas
Author:: Madhoo, Manisha
~
Title:: A Physician’s Guide to Helping Patients with ADHD Find Success in the Workplace
Year:: 2011
Citekey:: maoPhysicianGuideHelping2011
itemType:: journalArticle
Journal:: Postgraduate Medicine
Volume:: 123
Issue:: 5
Pages:: 60-70
DOI:: 10.3810/pgm.2011.09.2460
LINK
Abstract
The impact of untreated adult attention-deficit/hyperactivity disorder (ADHD) in the workplace can be substantial, and employees with ADHD often confront frustration, employer disappointment, and low performance ratings. As a result, adults with ADHD may seek treatment from primary care providers to improve occupational performance. Previously considered a behavior disorder primarily affecting children and adolescents, ADHD in adulthood presents primarily as a cognitive disorder. Self-management deficits play a greater role in adult ADHD, particularly with respect to occupational and interpersonal functioning. Although specialized resources are available to assist adults with ADHD, many afflicted individuals may be unaware or unable to access them. Primary care providers who may be treating adults with ADHD are in a unique position to help them obtain the care and support needed to build appropriate skills and manage occupational issues. In this review, a literature search of the past 10 years was conducted to identify articles concerning ADHD and its impact on individuals in the workplace. The influence of ADHD on occupational functioning is discussed in the context of self-management impairments, diagnosis and assessment, and management strategies. With early and successful intervention, adults with ADHD may be able to become more aware of the impact of ADHD on work performance and achieve successful occupational experiences. .
Notes
# Dum Dum Note
Test note
Jeremy’s Review
This paper is a literature review, particularly looking at papers published between 2001 and 2011 to help physicians better understand and mitigate the problems that arise from patients with ADHD in regards to their occupations. As primary care physicians are usually the first people a person may seek out for help, it is imperative that providers are able to understand the problem and know what resources to give them. It has been 12 years since this study was published and it is possible that the advancements in understanding ADHD may be further along.
Annotations
Imported: 2023-10-23 1:00 pm
Quote
Attention-deficit/hyperactivity disorder (ADHD) is a chronic condition affecting an estimated 4.4% of adults aged 18 to 44 years.1
Pg.2
*
Quote
Diagnostic criteria for ADHD are outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)3; however, these are based on symptoms in children and do not account for how these symptoms may change in adulthood. Although hyperactivity diminishes as children progress into adolescence and adulthood, symptoms of inattention remain.4
Pg.2
- How do these change? Look up Dr. Russell for this information
Quote
Release of DSM-V criteria, anticipated in 2013, are expected to more accurately reflect the symptoms and impact of ADHD observed in adults.6
Pg.2
*
Quote
In a national survey of US adults, those with self-reported ADHD had a higher divorce rate than age- and gender-matched controls without ADHD10; furthermore, adults with ADHD have a 50% likelihood of having a child with the condition,8,11 which may increase family and relationship difficulties
Pg.3
- Having ADHD is hard. It affetcs all facets of life and if you have others in the family with it (like kids) it creates a different set of problems.
Quote
In a large Norwegian study of 414 adults with ADHD and 357 controls, Halmoy et al16 found that factors such as presence of combined and inattentive ADHD subtypes; high scores on childhood and current ADHD symptoms; and reported anxiety, depression, and/or drug and alcohol abuse were strong predictors of unemployment. Conversely, early recognition and treatment of ADHD during childhood was a strong predictor of active work status in adulthood.
Pg.3
*
Quote
Although trained mental health professionals and career counselors are available to help adults cope with the symptoms and comorbidities of ADHD and guide them toward careers in which they can be successful, patients may not be able to find a counselor with these skills.4 Primary care providers, who serve as a home base for patient-centered medical issues, are concerned with the overall well-being of the patient and the patient’s family. Thus, they are well suited to help adults with ADHD obtain the care and support they need through early and successful intervention and referrals to community resources to help them build the appropriate skills and manage occupational and other issues
Pg.3
- Just as medical doctors can intervene early in equippoing and resourcing people to be successful in their health, we as the church can be (and should be) quick to help people who are called to serve God with appropriate resources.
Quote
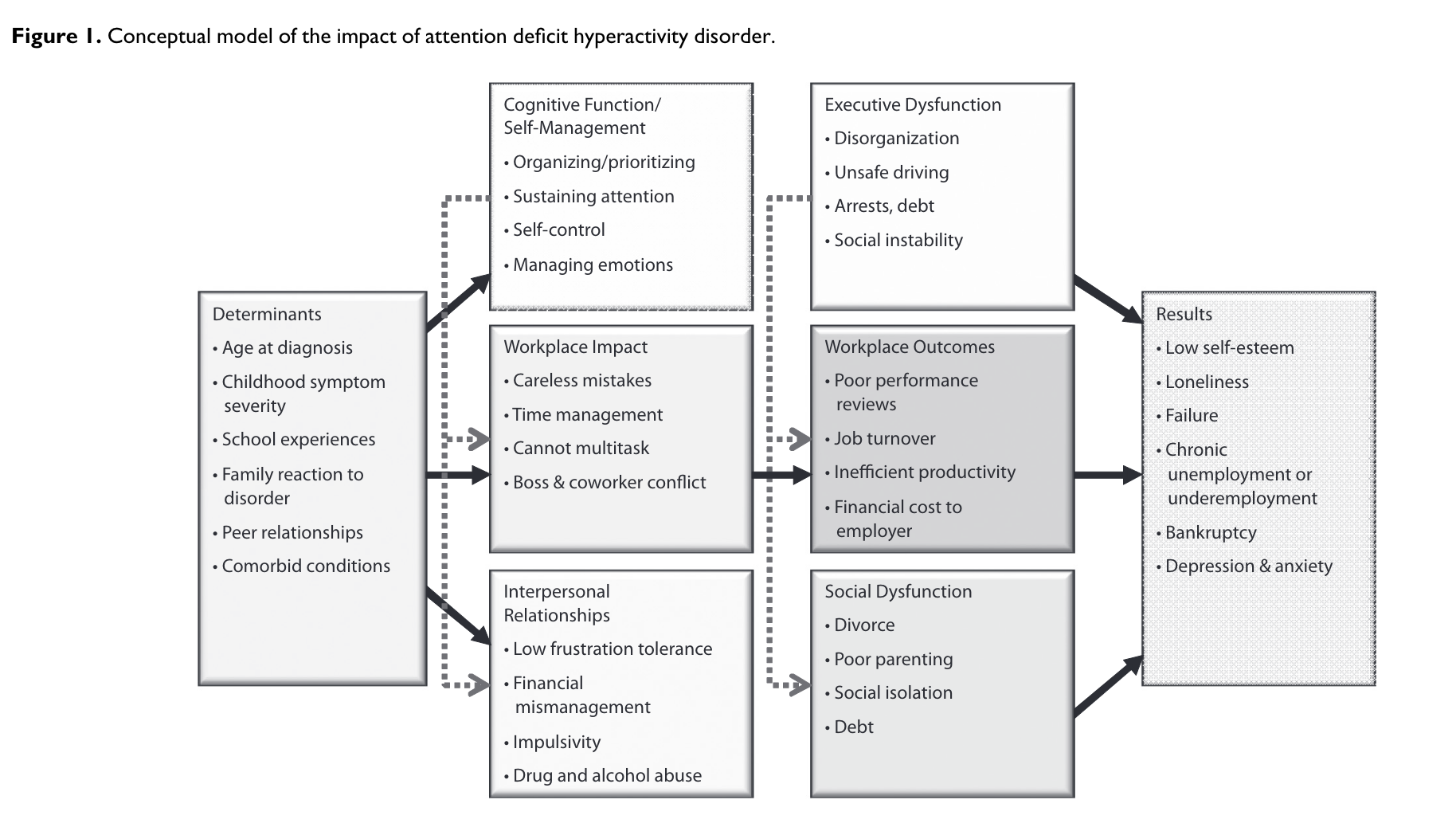
While ADHD was once considered a behavior disorder, it is widely recognized that many individuals with ADHD do not Cognitive Function/ Self-Management • Organizing/prioritizing • Sustaining attention • Self-control • Managing emotions Workplace Impact • Careless mistakes • Time management • Cannot multitask • Boss & coworker conflict Interpersonal Relationships • Low frustration tolerance • Financial mismanagement • Impulsivity • Drug and alcohol abuse Results • Low self-esteem • Loneliness • Failure • Chronic unemployment or underemployment • Bankruptcy • Depression & anxiety Determinants • Age at diagnosis • Childhood symptom severity • School experiences • Family reaction to disorder • Peer relationships • Comorbid conditions Executive Dysfunction • Disorganization • Unsafe driving • Arrests, debt • Social instability Workplace Outcomes • Poor performance reviews • Job turnover • Inefficient productivity • Financial cost to employer Social Dysfunction • Divorce • Poor parenting • Social isolation • Debt Figure 1. Conceptual model of the impact of attention deficit hyperactivity disorder
Pg.3
*
 maoPhysicianGuideHelping2011-3-x103-y523.png
maoPhysicianGuideHelping2011-3-x103-y523.png
Pg.3
*
Quote
have significant behavioral problems; instead, their difficulties center around an inability to focus on tasks and use working memory.17
Pg.4
- ADHD and behavior. Which causes which? Is ADHD make you bad alone, or is it the frustration of not being able to regulate your brain?
Quote
An alternate view is that all patients with ADHD have developmental self-management dysfunction, although this may not be immediately apparent. According to this model, impairments in self-management are most accurately assessed based on an individual’s real-life performance over time rather than neuropsychological tests conducted in a clinic under controlled conditions and over brief durations.20,24
Pg.4
- People can pass ADHD attention tests if the focus is there. Observations over time are likely a much better indicator of the depth of the self-management dysfunction of an individual.
Quote
In a US survey of mental disorders among 2399 adults residing in English-speaking households, ADHD was associated with an average of 35 days of lost work productivity annually, due either to absenteeism or to low performance while at work, with more lost work among blue collar workers than professional, technical, or service employees.29
Pg.5
- So many hours lost in productivity!
Quote
A study by Canu et al30 found that across several contexts, particularly work and academics, undergraduate students were significantly more reluctant to interact with young adults with ADHD than with those with other minor medical problems or an ambiguous weakness (eg, the perfectionist). These findings are consistent with a stereotypical perception that individuals with ADHD have impaired brain functioning and an inability to concentrate,31
Pg.5
- It is important to have a thick skin to be open about ADHD. It will likely negatively impact people’s perception about you.
Quote
In adults, the most common comorbid conditions with ADHD include substance abuse/dependence, mood disorders, and anxiety disorders;39 one epidemiologic survey reported lifetime comorbidity rates of 15.2%, 38.3%, and 47.1%, respectively.1
Pg.6
*
Quote
The misconception that ADHD is outgrown and does not need to be treated in adulthood may also impede diagnosis, as this belief inhibits a patient–physician dialogue about current or past ADHD symptoms. It is also important to recognize that adults with a history of professional achievement and/or high IQ who were previously able to adequately compensate for ADHD challenges4 may now encounter impairments as increasing demands surpass their coping skills.
Pg.6
- It is important to recognize that someone who has made it to the point of being a professional (in this case a clergy member) that there has been some forms of modifications and accommodations (intentionally or not). This does not remove the need for intervention by trained professionals to assist someone with an ADHD diagnosis.
Quote
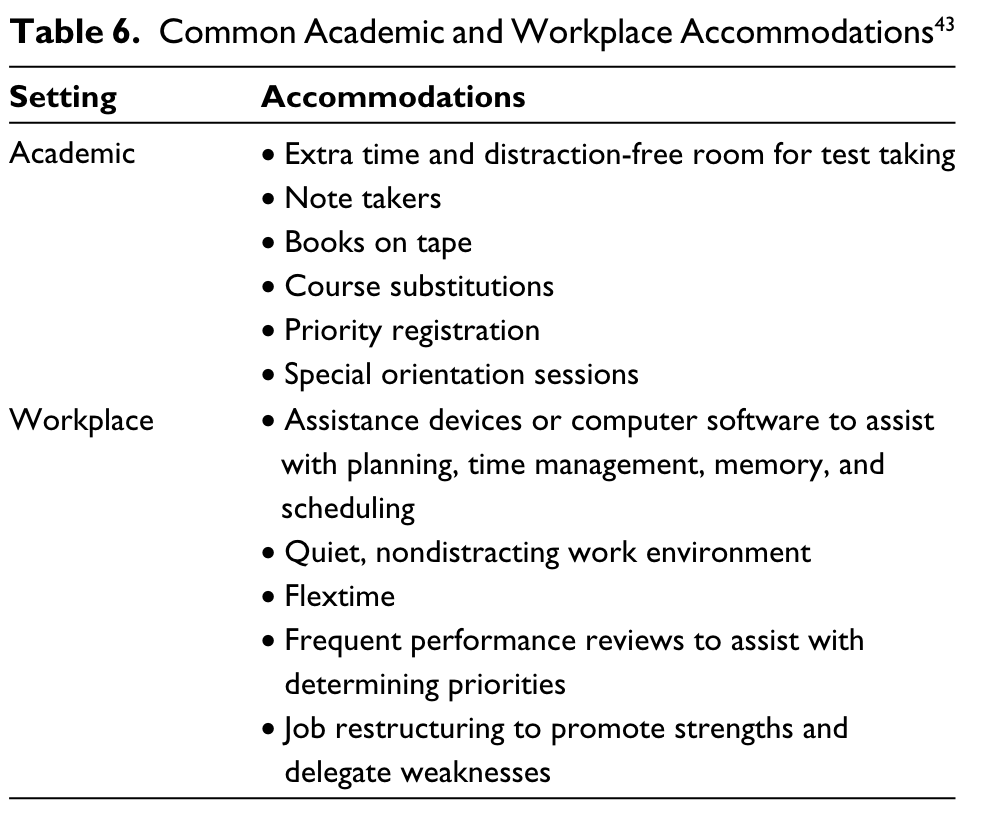
However, ADHD is a condition in which multiple domains of life are impacted, and such criteria do not necessarily account for the impact of daily work and personal demands that may have brought the patient to the office. Management of adult ADHD, therefore, may require a multimodal approach that combines pharmacologic, cognitive, and behavioral therapies,43–45 and it should be treated as a lifelong disability, similar to other manageable conditions such as diabetes.43
Pg.6
- ADHD is a a lifelong disability that will require a multi-faceted approached. ADHD affects everything, therefore it should always be managed using appropriate interventions.
Quote
Personal coaching is an emerging treatment for adults with ADHD. This approach differs from psychotherapy in that it focuses on results-oriented action rather than insight. Coaches help individuals with ADHD set realistic goals, devise strategies to reach those goals, and provide motivation to keep individuals on course.43 However, there is currently limited systematic research to support the treatment.
Pg.7
- I think a lot of people will understand their struggles at a certain point and the limitations that they impose. At that time, perhaps setting goals and working towards them gives the incentive to put practices into place.
Quote
Each individual with ADHD has different strengths, weaknesses, intellectual abilities, and severity of impairment. Thus, a successful management plan should center on individual needs and goals.
Pg.9
- It is always important to remember that at the end of the day, everyone is unique. There may be many commonalities because of certain ailments or disorders, but it doesn’t change the individuality of the person.
 maoPhysicianGuideHelping2011-9-x100-y228.png
maoPhysicianGuideHelping2011-9-x100-y228.png
Pg.9
*
 maoPhysicianGuideHelping2011-9-x355-y572.png
maoPhysicianGuideHelping2011-9-x355-y572.png
Pg.9
*
Quote
The detrimental impact of ADHD in the workplace can be substantial, but may be mitigated with successful intervention.
Pg.10
*
Quote
Although interventions initiated for ADHD later in life may not necessarily result in the same level of success observed during childhood,16 treatment in adulthood is critical to avoid the ongoing impact ADHD may have on the individual’s quality of life.
Pg.10
- The best time to start the management of ADHD is in childhood, but the next best time is now.
Quote
1. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163(4):716–723.
Pg.10
*
Quote
4. Nadeau KG. Career choices and workplace challenges for individuals with ADHD. J Clin Psychol. 2005;61(5):549–563.
Pg.10
*
Quote
6. Kessler RC, Green JG, Adler LA, et al. Structure and diagnosis of adult attention-deficit/hyperactivity disorder: analysis of expanded symptom criteria from the Adult ADHD Clinical Diagnostic Scale. Arch Gen Psychiatry. 2010;67(11):1168–1178.
Pg.10
*
Quote
8. Adler L, Cohen J. Diagnosis and evaluation of adults with attentiondeficit/hyp
Pg.10
*
Quote
11. Faraone SV. Genetics of adult attention-deficit/hyperactivity disorder. Psychiatr Clin North Am. 2004;27(2):303–321.
Pg.10
*
Quote
16. Halmoy A, Fasmer OB, Gillberg C, Haavik J. Occupational outcome in adult ADHD: impact of symptom profile, comorbid psychiatric problems, and treatment: a cross-sectional study of 414 clinically diagnosed adult ADHD patients. J Atten Disord. 2009;13(2):175–187.
Pg.11
*
Quote
17. Brown TE. ADD/ADHD and impaired executive function in clinical practice. Curr Psychiatry Rep. 2008;10(5):407–411.
Pg.11
*
Quote
20. Brown TE. Executive functions and attention deficit hyperactivity disorder: Implications of two conflicting views. Int J Disabil Dev Edu. 2006;53(1):35–46.
Pg.11
*
Quote
24. Barkley RA. ADHD and the Nature of Self-Control. New York, NY: Guilford Press; 1997.
Pg.11
*
Quote
29. Kessler R, Adler L, Ames M, et al. The prevalence and effects of adult attention deficit/hyperactivity disorder on work performance in a nationally representative sample of workers. J Occup Environ Med. 2005;47(6):565–572.
Pg.11
*
Quote
31. Schmitz MF, Filippone P, Edelman EM. Social representations of attention deficit/hyperactivity disorder, 1988–1997. Culture Psychology. 2003;9:383–406.
Pg.11
*
Quote
9. Kolar D, Keller A, Golfinopoulos M, et al. Treatment of adults with attention-deficit/hyperactivity disorder. Neuropsychiatr Dis Treat. 2008;4(1):107–121.
Pg.11
*
Quote
43. Murphy K. Psychosocial treatments for ADHD in teens and adults: a practice-friendly review. J Clin Psychol. 2005;61(5):607–619.
Pg.11
*
Quote
44. Knouse LE, Safren SA. Current status of cognitive behavioral therapy for adult attention-deficit hyperactivity disorder. Psychiatr Clin North Am. 2010;33(3):497–509.
Pg.11
*
Quote
45. The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Arch Gen Psychiatry. 1999;56(12):1073–1086.
Pg.11
*